

to
Global health is an important field that the three of us wanted to gain experience within. We therefore contacted the department of global health in Bergen with a wish to travel abroad. After some planning we were ready to travel to Lahore in Pakistan January 2023 for a three week long internship through NORPART.
In Lahore we were accommodated at LUMS, Lahore University of Management and Sciences. At campus we met a lot of students and professors doing research in different fields, among them biochemistry and microbiology. We were given a warm welcome and a tour in the laboratory and the students told us about their projects. We got a great impression of Pakistan and its very hospitable people!

During our two week internship we visited Gulab Devi Chest hospital (a charity hospital), the Children’s hospital (a public hospital), Medixs hospital (a private clinic funded by Smile Train) and Shalimar hospital (a charity and private hospital). As our stay was so short and not much planned beforehand, the departments we visited were much dependent on our interests. The hospitals were very accommodating to meet our wishes.

At the Children’s hospital we visited the plastic surgery department, HDU, and participated in NORPART’s project on Tuberculosis and nutrition. A plastic surgeon at the Children’s hospital also invited us to visit his clinic at Medixs hospital in the evening to see cleft lip and palate surgeries.
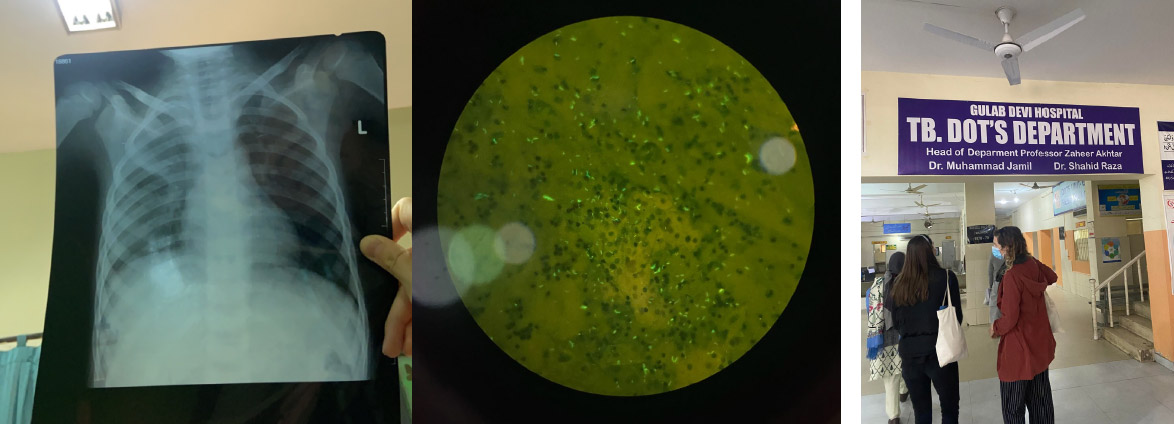
At Gulab Devi we visited the departments and wards of interventional cardiology, CCU, gynaecology, pulmonology, tuberculosis, ICU and general surgery. At Shalimar we got a general tour of the hospital and also visited the outpatient clinics of pulmonology and gynaecology, microbiology, the private rooms in the medical wards and the emergency unit.

We were not sure what to expect from this stay and we only got to visit the hospitals for two weeks. However we feel that we have learned a lot. It seems as though the education of medical doctors in Pakistan is really good, and this is reflected in the knowledge of the doctors we met. They were very eager to teach us about the patients and to explain the procedures. We always felt welcome to any department and were able to ask questions at any time. Even though we were not able to perform any medical procedures or participate in the treatment as we don’t have a licence to practise medicine in Pakistan, and due to language barriers, we were able to observe and examine the patients. In the wards the doctors gave patient histories during rounds and we could investigate the findings if relevant. It was very interesting to see diseases that are not common in Norway and also the result of not contacting the health care in time with common diseases such as breast cancer. The treatment however, was relatively similar to the one at home with minor differences depending on i.e. resources available and the microbiological environment.
The lack of resources seems to be the main problem in the health care system in Pakistan. It was really devastating to see several really ill children in overcrowded beds while the doctors were running around and did not have the resources to help. The same patients would have received the necessary treatment in Norway, and in private hospitals in Pakistan. At the high dependency unit they did not always have a defibrillator available for resuscitation. Even at Shalimar a patient had to be transferred to a different hospital as they did not have available ventilators. At the gynaecological department we were able to see a vaginal delivery. Also here the women shared the same beds. We were told that they were not able to run one of the operating theatres due to lack of personnel.

The distribution of doctors versus midwives was very different from home. We were told that Pakistan does not have a lot of nurses or midwives because women instead are housewives. They do however have an abundance of doctors. This is very different from Norway and other Western countries. The result is that the tasks of the doctors and nurses vary from Norway. We even observed that parents and family did a lot of monitoring and treatment of the patients, such as ventilating their critically ill children.
It was also difficult to understand the systems in the hospitals. In the emergency rooms they had a triage system, but not in the outpatient clinics. A system of patient records was not available, and the patients had to bring their papers with them from previous hospital stays. Hand written notes were the norm, and all the radiological pictures were printed. At Shalimar they had an established system for patient records.
The disease burden is also affected by lack of knowledge of general health among the patients, especially among the population in the rural areas. A focus on preventive health such as general hygiene, guidelines for overuse of over-the-counter-antibiotics and nutrition could be useful to reduce hospital admissions. Also in the hospitals the infection prevention could be improved. It was hard to find hand sanitizer, gloves and masks, and the toilet facilities both for patients and employees were lacking. Patients with infectious diseases such as Tuberculosis were not isolated properly. The personnel did not use uniforms, only at the surgical departments, and also there the uniforms were mostly private. The equipment was often reused, and not always properly sterilised. A focus on hygiene and a decrease in use, especially incorrect/misuse, of antibiotics will definitely contribute to better health in general, and less pressure on the health care system in particular. The above mentioned actions will over time, in addition, make a big difference in the decreasing of hospitalacquired infections, something that is a frequent problem in Pakistan, as well as an increasing problem in global health perspective. But again, these measures require resources that unfortunately lack in Pakistan's health care system as the situation is today.
Another issue we became aware of was presented when we asked the doctors about clinical research. The healthcare system lacks a database for registering information about the population. As a consequence there is little data about prevalence of disease, and exact knowledge about the outcome of a given treatment in the Pakistani population. To collect data of prevalence in the population could be useful in the future and might be something NORPART can contribute to. Treatment is, as far as we noticed, based on global evidence based research. The medical doctors are very skilled in their fields, but the use of clinical research adapted for the population in Pakistan needs to increase.
We also travelled to the Norwegian embassy in Islamabad to talk about the NORPART project. They were all really interested in our experience with the Pakistani health care system, what we learned from our visits at the hospitals and what impressions we will take with us back to Norway. In addition we also get to tell them about our overall impression of Pakistan, such as the lovely and welcoming people, the delicious food, the beautiful nature and interesting history.

To conclude: we met a lot of kind, smart and helpful people on our travels. Everyone was very incredibly hospitable! Our experience with the NORPART project has been very positive, and we will take all the impressions and the knowledge with us throughout our future medical career. We definitely hope that our experience can inspire other students to travel to Pakistan through this project, and this is something that we will strongly recommend to anyone who asks. This is an experience for life where you don't only get to learn about your field of education, but also a different culture and a different way of life! Our overall impression with the health care system in Pakistan, is that the doctors and other personnel are highly educated and skilled, as well as hardworking and ambitious. They all are eager to contribute to the national, as well as, global health system. However the lack of resources, due to lack of governmental funding, lays the foundation of a health care system in trouble. This leads to poor patient treatment with huge differences based on socioeconomic status, lack of basic systems and necessary equipment, as well as failure in preventive health, hygiene and misuse of antibiotics. We all aspire to continue working with health from a global perspective and we hope that the NORPART project will facilitate a better collaboration across borders and contribute to development within health, education and research.